
Uses of Compressed Spectral Array in Intensive Care
1) Depth of Sedation
The normal awake EEG is dominated by alpha waves (frequency 8 – 13Hz). When sleepy or moderately/deeply asleep theta (4-7Hz) and delta (<4Hz) waves dominate the EEG respectively. Sedation produces a similar effect to sleep by reducing the frequency of the brain waves. It is important to note that during the initial stages of sedation, the amplitude or power of the EEG waves are expected to increase (due to presence of larger slow frequency waves), but then should decrease as sedation is deepened due to suppression of brain activity.
Trends in the level of sedation can be followed by monitoring the SEF. An SEF of 7 – 8Hz is the normal target for most intensive care patients as this is associated with ‘normal sleep’ levels of sedation. Occasionally deeper levels of sedation may be required e.g. refractory status epilepticus or raised ICP in traumatic brain injury and in these situations burst suppression is normally targeted. At this deep level of sedation brain wave activity is deeply suppressed with intermittent bursts of high frequency activity. On the CSA burst suppression is indicated by intermittent breaks in the solid SEF line. As there are sudden bursts of high frequency activity the value for the SEF will actually increase with burst suppression compared to deep sedation without burst suppression (the value of SEF is burst suppression doesn’t reflect the level of sedation).
Examples
a) No sedation – note the predominance of alpha and beta waves on the raw EEG with high frequency (SEF1 = 11 Hz, SEF2 = 16 Hz) activity.

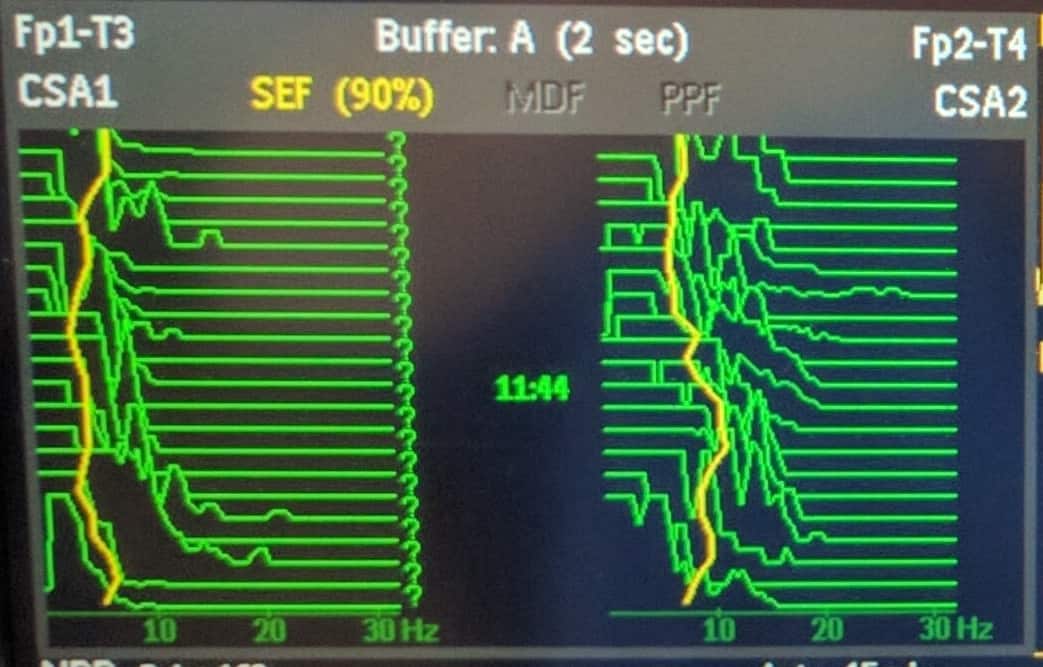
b) Moderate Sedation – note the moderate values for frequency (SEF1 = 5 Hz, SEF2 = 7.5 Hz).
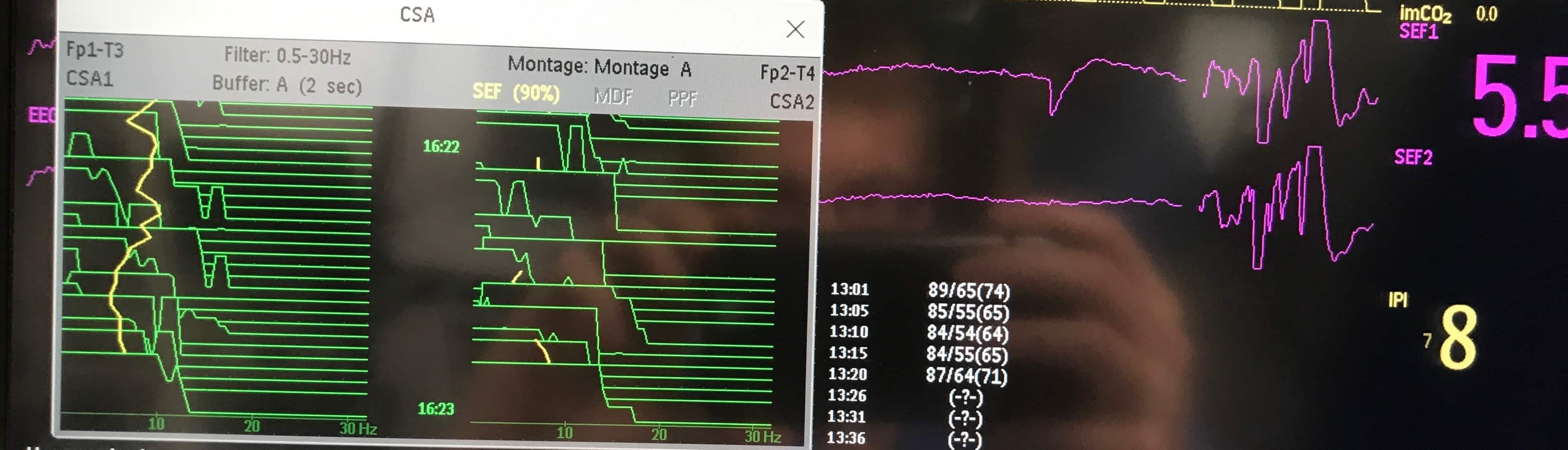
c) Deep sedation – note the predominance of delta waves on the raw EEG with low values for frequency (SEF1 = 1.5 Hz, SEF2 = 1 Hz).

d) Burst Suppression – note flat EEG with bursts of high frequency activity and the breaks in the yellow SEF line on the CSA.
2) Seizure activity
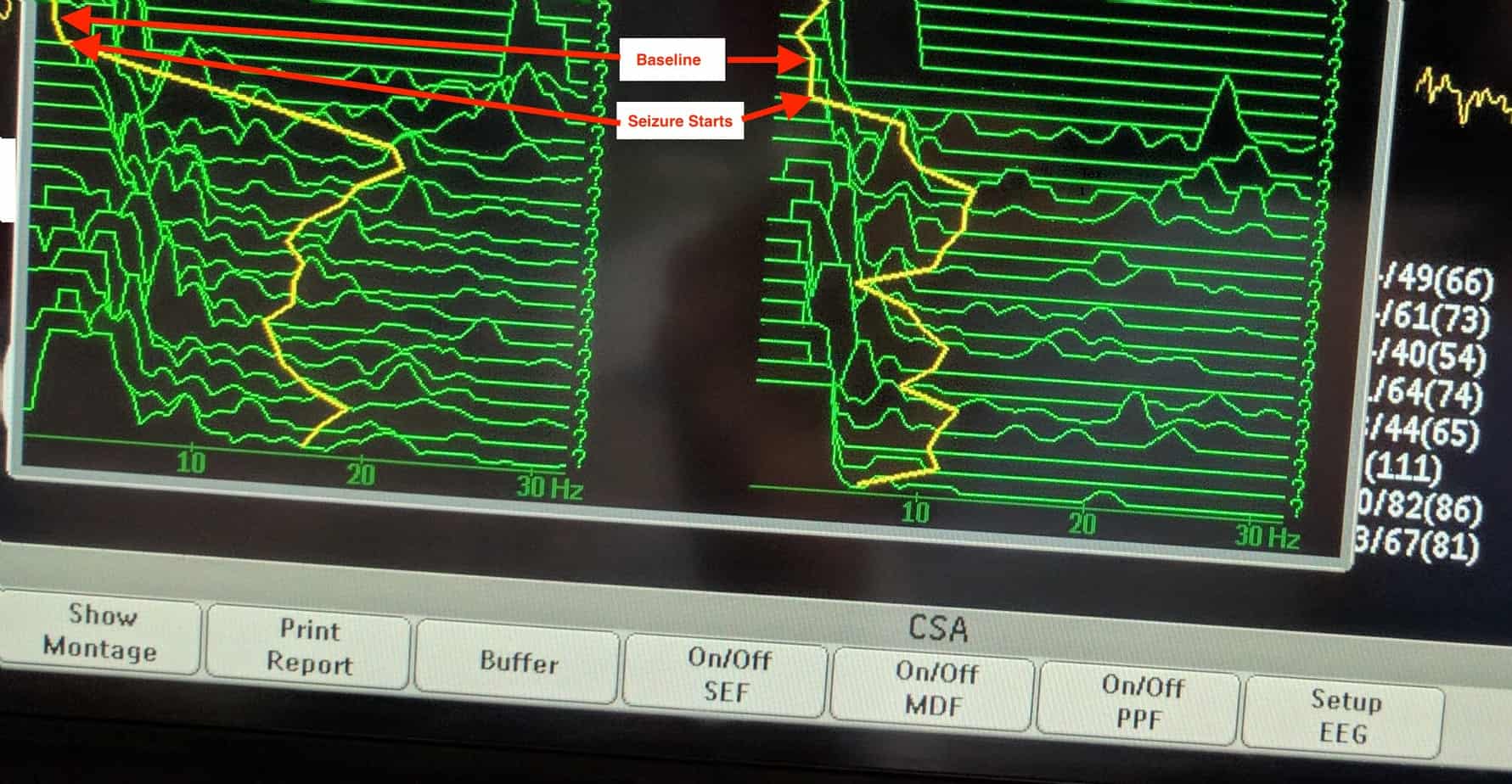
Seizure activity is associated with a sudden increase in high frequency, high power activity (the SEF line makes a sudden deviation from it’s baseline to the right hand side associated with an increase in total power). Movement artefact may mimic seizure activity on CSA, so it is important that the patient isn’t moving or stimulated during the interpretation. It is common for the frequency on the CSA to increase with patient stimulus, however the power doesn’t normally increase with this (the high frequency waves associated with an increased level of consciousness have a lower power).
Examples
a) Generalised Seizure Activity – note sudden increase in frequency from baseline (movement of yellow SEF line and peaks to right) with increase in power (height of peaks).
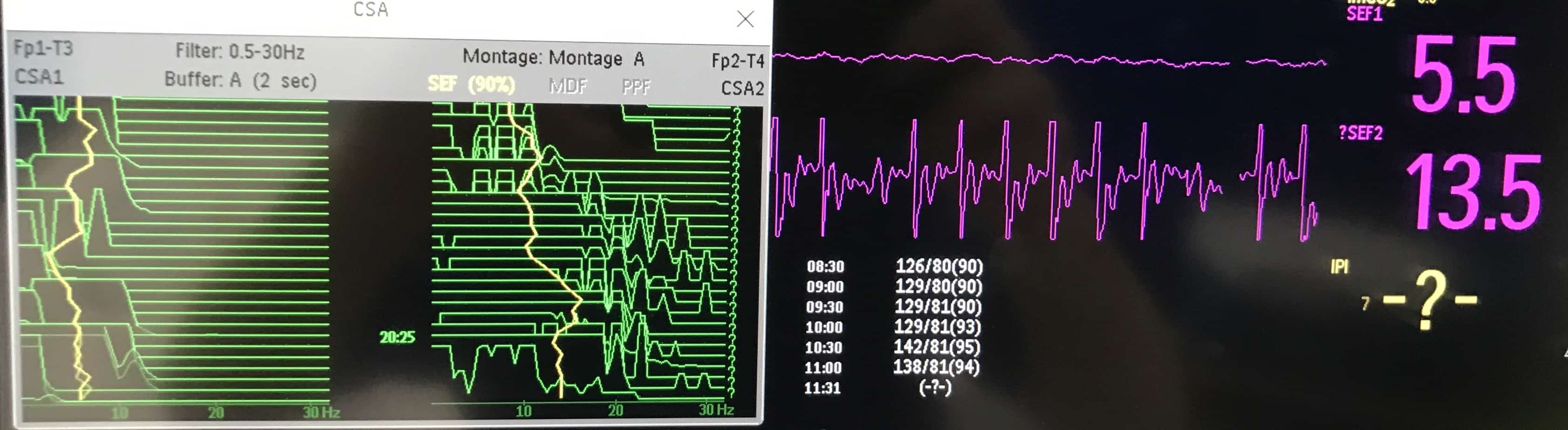
b) Focal Seizure Activity – note sudden onset asymmetry between the two sides which had previously been symmetrical (note the increased frequency and power on the right sided CSA, which was associated with left sided clinical seizures).
3) Regional blood flow
As the CSA displays activity from both sides of the brain side by side, differences between the two sides are normally obvious. The effects of sedation normally produce global changes in brain wave activity, with both sides equally effected, therefore producing symmetrical changes on CSA. Asymmetry on CSA can be due to focal seizures (sudden onset of high frequency, high power activity) or can be due to cerebral ischaemia (reduced cerebral activity with reduced frequency and power). Cerebral ischaemia in PICU is often caused by external compression e.g. haemorrhage in traumatic brain injury or cerebral oedema, however interruption of blood supply due to thrombus will produce a similar effect.
Indications for using CSA in Intensive Care
- Any patient at risk of non-convulsive status epilepticus e.g. post arrest patient, traumatic brain injury or patient with epilepsy requiring administration of a muscle relaxant infusion etc
- To helps titrate level of sedation to targeted level e.g. burst suppression
- Patients with possible seizure activity (helps determine if abnormal movements or clinical signs are due to seizure activity)
Conditions for Use
Movement artefact makes the CSA difficult to interpret and therefore analysis or documentation of values should not be made in an active patient – consider increasing the level of sedation or administration of muscle relaxants to facilitate accurate recording if the clinical question warrants it use.
![]()